Spasmolytic action. Antispasmodics
Yu. Belousov, Dr. honey. sciences, prof.
Spastic reactions accompany a significant number of diseases.b In this
Due to this, symptomatic antispasmodic therapy becomes very relevant.
Antispasmodics are widely used in diseases of the gastrointestinal tract, in
in particular with irritable bowel syndrome, with urological diseases,
spastic dyskinesias in gynecology.
Asthma has increased in recent years and is characterized by hyperresponsiveness and inflammation of the airways. Many patients report using alternative methods treatments for self-treatment of asthma symptoms as adjuncts to short-acting and long-acting β-agonists and inhaled corticosteroids. Up to 40% of asthma patients use herbal therapies to treat asthma symptoms, often with no proven efficacy or known mechanisms of action.
Therefore, it is important to study both the therapeutic and possible negative effects of the isolated components of herbal treatments on Airways. We assumed that ginger and its active ingredients cause bronchodilation by modulating intracellular calcium in airway smooth muscle.
Table. Classification of myotropic antispasmodics
To myotropic antispasmodics, or myolytics, which are widely used,
include: drotaverine (no-shpa), mebeverine, papaverine, otilonium bromide.
Myolytics lower smooth muscle tone by directly influencing biochemical
intracellular processes. They either lead to an increase in intracellular cAMP
or decrease in intracellular cGMP. cAMP activates the release of Ca++ from the cell and its
deposition, which leads to a decrease in the contractility of the cell. cGMP,
on the contrary, it increases contractility due to the stimulation of the release of Ca ++ from the depot.
Key words: asthma, lungs, herbal, botany, bronchodilation. In recent years, the prevalence of asthma has steadily increased and is characterized by bronchospasm, increased airway hypersensitivity, and airway inflammation. In addition to conventional asthma therapy, namely short-acting and long-acting β-agonists and inhaled corticosteroids, many patients report using complementary and alternative medicine to self-manage asthma symptoms.
Natural herbal products in the form of teas, topical ointments and nutritional supplements have received accolades for relief respiratory diseases including cough and bronchospasm. An estimated 40% of asthma patients use herbal therapies to self-medicate their asthma symptoms. Of note is the use of ginger to relieve respiratory symptoms, dyspepsia, and gastrointestinal motility disorders. In addition, we hypothesize that the purified components of raw ginger, namely -hegerol, -hegerol, -hegerol, and -shogaol, will relax airway smooth muscles and potentially serve as novel bronchodilators.
Papaverine is an opium alkaloid that has a myotropic antispasmodic effect on
smooth muscles of the intestines, bile ducts and urinary tract, especially
with spasms. Unlike other alkaloids, opium does not affect the central nervous system.
According to modern concepts, papaverine inhibits phosphodiesterase (PDE) in muscles,
which leads to an increase in the concentration of cAMP and associated with its accumulation
relaxation smooth muscle. On the other hand, papaverine tends to
action similar to calcium antagonists.
In diseases such as asthma, the hypercontracting phenotype is partly due to an imbalance of these factors. Airway smooth muscle contraction is regulated, in part, by intracellular calcium. With a better understanding of the mechanisms by which the purified components of ginger affect the respiratory tract, we can explore the use of these natural herbal remedies to relieve asthma symptoms.
Cultured muscle cells with human breath
Detailed methods are provided in the online application. Animal protocols have been approved by the Columbia University Animal Care and Use Committee. The male guinea pigs were anesthetized and their tracheas were removed. Experiments using human surgical waste were reviewed by Columbia University's Institutional Review Board and considered acceptable as "non-human research". Smooth muscle tissue was carefully dissected, and the epithelium was removed. The strips were fixed in the organ bath as described in the online application.
Papaverine has a maximum antispasmodic effect on the colon, further
in descending order of effect: on the duodenum, antrum.
Papaverine is well absorbed from the gastrointestinal tract, may accumulate
in the liver and adipose tissue, extensively metabolized in the liver by microsomal
enzymes by conjugation with phenol, further excretion is carried out
by the kidneys by 60% in the form of metabolites, the rest is excreted unchanged.
Preliminary problems with contracts
In an online supplement.
Airway resistance measurements
Three baseline measurements were taken followed by pre-treatment either with vehicle control or with 100 μM messerol delivered via a 10 second spray. For these experiments, 15 guinea pigs, 10 human samples and 25 mice were used. However, not all protocols were followed in every animal or sample. The values given in the figure results and legends are the number of animal or tissue samples.Side effects: nausea, anorexia, diarrhea or constipation, malaise, headache
pain, dizziness, allergic skin reactions, rarely jaundice. At
parenteral administration, papaverine disrupts atrioventricular conduction and
can cause heart block.
Drotaverine (no-shpa) - antispasmodic myotropic action; on
activity is superior to papaverine.
Raw ginger relaxes the human respiratory tract Smooth muscle
The values for cellular data are the number of days the experiments were run. Bonferroni's correction was applied for multiple comparisons. Conventional human tracheas with epithelium removed were suspended in an organ bath and infected with acetylcholine. With stable force generation, an increase in the amount of food grade ginger powder suspended in 1 ml of water was added to the Krebs-Hensleit buffer, and the water was used as a vehicle control.
The mechanism of action of drotaverine has been studied for many decades. He
associated with a change in the intracellular content of cyclic adenosine monophosphate
(cAMP) - a regulator of muscle tone. Drotaverine blocks a specific enzyme
phosphodiesterase, which degrades cAMP. Recent studies have shown that
PDE enzyme is represented by numerous isoenzymes (PDE I-VII), which
are located in different tissues and perform different functions. Drotaverine has
the highest selectivity of action against PDE IV (cAMP-sensitive), which
and is manifested by the accumulation of intracellular cAMP and a decrease in contractile
cell abilities. In addition, drotaverine has other mechanisms of action:
has the effects of calcium antagonists, blocks Na + channels (table). Together with
meanwhile, drotaverine is completely devoid of anticholinergic activity. Therefore, among
of all known groups of antispasmodics, no-shpa is one of the most
safe and well tolerated drugs.
These studies were repeated in human tracheas obtained from 4-7 different donors. However, not all compounds were tested in every sample. However, new aspects of the present work include the study of -hekerol, -hegerol, -gengerol and -shogaol as unique bronchodilator compounds.
Collectively, these data include the first indications of mechanical signs of ginger's broncho-axicatory properties and confirmation that -hexerol, -hexerol and -shogal, but not -hegerol, are the active components of this phytotherapist responsible for bronchorelaxation. With up to 40% of asthma patients self-treating asthma symptoms with herbal remedies, it is becoming increasingly important to understand the active components of these herbal therapies, their mechanisms of action, and potential interactions with current asthma therapy.
After oral administration, drotaverine is well and rapidly absorbed, bioavailability
is 65%, and the maximum concentration in the blood is reached within 1 hour.
Drotaverine is highly associated with plasma proteins (95-98%); volume
distribution is large. Drotaverine penetrates well into various tissues: the central nervous system,
adipose tissue, myocardium, lungs, kidneys, liver, wall of the urinary and bile
bladder, intestines, vascular wall. Elimination is carried out slowly, per day
about 25% of the substance is eliminated, which is the result of the biliary pathway
excretion (up to 50%) and the presence of enterohepatic circulation. Drotaverine completely
metabolized in the liver with the formation of numerous metabolites. Period
half-life is 16 hours.
The authors acknowledge Dr. Alison Rinderspracher's insight and contributions to the chemical structure and sites of activity of ginger components. Herbal treatments for asthma: a systematic review. The role of phytochemicals in bronchial asthma. The medicinal herb is used among asthma patients attending a specialized treatment service in Trinidad.
Herbals and asthma: patterns of use in the population. Inhibitory effect of inhaled complex traditional Chinese medicine on early and late asthmatic reactions induced by ovalbumin in sensitized guinea pigs. Efficacy and tolerability of antibiotic drug therapy in adult patients with moderate to severe allergic asthma.
In order to improve the drug, a new dosage form -
no-shpa forte, with a high content of drotaverine hydrochloride (80 mg).
Side effects: with the introduction of a feeling of heat, sweating, dizziness,
tachycardia.
Antispasmodics of myotropic action also include calcium antagonists.
Calcium antagonists have an antispasmodic effect by blocking
slow voltage-gated calcium channels in smooth muscle
gastrointestinal tract.
Usage folk remedies among patients in Karachi Pakistan. The stability of gingerol and shogaol in aqueous solutions. Ginger-chemistry, technology and quality assessment: part 2. Pharmacokinetics of 6-gingerol, 8-gingerol, 10-gingerol and 6-shoogal metabolites and conjugate in healthy people.
He names smooth muscle to represent his actin and myosin myofilaments in a different position from that of the skeleton, without striations. Smooth muscle is divided into two morphological types: unitary or visceral smooth muscle and multipurpose smooth muscle.
Calcium antagonists also have little effect on receptor-dependent calcium channels,
therefore, they have a predominant effect in the duodenum 12. About 40%
tonic contractions of the colon are resistant to calcium antagonists, tk.
are carried out due to the mobilization of Ca ++ from intracellular depots. Antagonists
calcium cannot block the release of Ca++ from the depot.
The first is formed by muscle cells grouped in a compact form, forming sheets or bundles surrounded by connective tissue. This is a typical formation of the muscular walls of hollow visceral structures. The second is isolated muscle cells, although they may be close to each other. They are part of the trabeculae of the spleen, etc.
They are smaller than corrugated. Units are low resistance bridges, giving them the functional characteristics of syncytial muscles. At these low resistance points, small pores are found where ions and small molecules pass through. These connections provide the electrical connection between these cells.
Of the calcium antagonists, the antispasmodic effect of verapamil is 2-3 times stronger,
than nifedipine or diltiazem. Verapamil has an antispasmodic effect in
12 duodenal ulcer in concentrations much lower than required for
implementation of cardiovascular effects. Antispasmodic efficacy
calcium antagonists significantly decreases in the direction from upper to lower
sections of the gastrointestinal tract.
They are formed by actin and myosin phytins that are more or less parallel to the longitudinal axis, although they do not show striations as in the skeletal one. Thin threads tend to surround thick threads. This high resistance reflects the low passive permeability for potassium and chlorine. According to the concentrations of these ions inside and outside, the equilibrium potentials according to the Nernst equation are 62 mV for sodium, -89 mV for potassium, and -22 mV for chlorine. The difference between the theoretical value and the real one can be explained by the presence of electrogenic pumps.
Currently, another myotropic antispasmodic with high
selectivity for the lower gastrointestinal tract - otilonium bromide.
Otilonium bromide (spasmomen) - myotropic antispasmodic, quaternary
ammonium compound, more active than papaverine. Mechanism of action of otilonium bromide
associated with the regulation of the level of intracellular Ca ++: it prevents both the entry of Ca ++
from the extracellular space, and blocks the mobilization of Ca ++ from the depot. This
the mechanism is of greatest importance in colonic contractions. Wherein
otilonium reduces both the amplitude and frequency of contractions, in contrast to
papaverine, which to a greater extent reduces the amplitude of contractions of the thick
intestines. Anticholinergic properties are weak and clinical significance not
have.
In addition to passive diffusion and these pumps, diffusion by exchange plays an important role in maintaining ionic concentrations. Here the sodium moves along its electrochemical gradient while the exchange or cotransport ion does so against its electrochemical gradient.
The required energy comes from the sodium electrochemical gradient. Its importance is under discussion. Perhaps there is a Sa bomb. This property also seems to depend on the assembly of the cell, as this could not be proven in isolated smooth cells.
Otilonium bromide, unlike all other antispasmodics, is
highly selective agent due to the peculiarities of pharmacokinetics.
It is practically not absorbed after oral administration; is not subject to absorption.
more than 5% of the drug and 97% is excreted unchanged through the gastrointestinal tract.
Therefore, otilonium bromide acts exclusively locally (in the intestines) and has no
no systemic effects, incl. side effects.
The duration of these rhythms is determined by the rate of prepotential depolarization and the distance between the threshold level and membrane potential. The possible involvement of enteric and non-therogenic hormones, as well as non-nervous myogenic factors, must also be considered.
These slow waves are in response to signals originating in axon plexuses that contain Cajal interstitial cells, which form tight junctions with smooth muscle and are not thought to be a product of the functional characteristics of muscle cells.
Otilonium bromide due to the mechanism of action is the most effective in
increased motor activity of the colon, which is more often observed in the syndrome
irritable bowel with diarrhea.
Otilonium bromide is prescribed 40 mg 2-3 times a day before meals.
Otilonium bromide has excellent long-term tolerance in contrast to
from other antispasmodic drugs.
Action potentials usually appear on these waves of depolarization propagated by an electric tone, waves that suffer from a reduction in their propagation. Likewise, possible bursts do not change the frequency or amplitude of these slow waves of depolarization.
The ionic mechanism involved has not yet been established, although it does know that there is an initial increase in sodium conductance and another cationic conductance is activated at -50 mV. The fact that a cell reaches its threshold of excitability with these waves of depolarization and generates action potentials depends on its excitability, which is determined by such important factors, as external or internal nerve influx, hormonal influx and the influence of myogenic factors.
Thus, clinicians have several antispasmodic agents at their disposal.
drugs with sufficient efficacy and a wide profile
security.
Antispasmodics(antispasmodics), lek. in-va, causing a decrease in tone or elimination of spasm of smooth muscles and ext. organs (gastrointestinal tract, bronchi, uterus, biliary and urinary tract, etc.). Spasmolytic. St. you have drugs that affect decomp. regulation of smooth muscle tone. There are neurotropic (act on the nervous system) and direct myotropic (act on muscles) antispasmodics, but some lek. in-va can be attributed simultaneously to both groups. Among neurotropic antispasmodics, central (, sedatives,) and peripheral (,) actions are distinguished.
These action potentials are highly variable in smooth muscle, ranging from fast bursts to very slow bursts, and sometimes these potentials can set in, giving rise to a long plateau phase. There is agreement that the action potential surge is due to calcium influx. However, there is a potassium output current that overrides the calcium input current, which is the cause of the former, causing the spike to be smaller than expected and which rarely reaches zero potential.
If calcium is low, the input current is maintained by sodium. Repolarization occurs due to the release of potassium, and this can occur on early stage in the depolarization phase, which avoids potential inversion. These action potentials are always superimposed on the ascending region of slow depolarization waves, although these waves are not necessarily accompanied by action potentials.
Spasmolytic. effect of antispasmodics center. actions associated with limiting the flow of nerve impulses from the center. nervous system to the performer authorities. Peripheral neurotropic antispasmodics block or stimulate the corresponding ones in the execution. organs and. For example, anticholinergic drugs lower the tone or eliminate spasm of the gastrointestinal tract with peptic ulcer stomach and duodenum; stimulators of b 2 -adrenergic receptors reduce spasm of bronchial muscles in obstructive bronchopulmonary diseases.
The mechanisms of action of myotropic antispasmodics have not been fully elucidated. It is believed that these drugs affect the biochem. and biophys. p-tion, accompanying muscle contraction and regulating the content of cyclic. in smooth muscle, movement of Na +, K + and Ca 2+, formation or release from tissue depots of endogenous biologically active in-in(, etc.), changing the tone of smooth muscles and ext. organs.
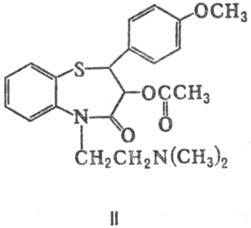
Spasmolytic. St. you also have drugs from the group of so-called. Ca 2+ antagonists. The mechanism of their action is associated with the ability to inhibit the entry into the smooth muscle of Ca 2+ necessary for muscle contraction and, in connection with this, lower myofibrillar, which leads to a decrease in the utilization of energy-rich muscles and, consequently, to its relaxation. Ca 2+ antagonists include derivatives of phenylalkylamine (eg, verapamil), dihydropyridine (, or; f-la I), benzothiazepine (; II), (, or, III; lidoflazin, IV).
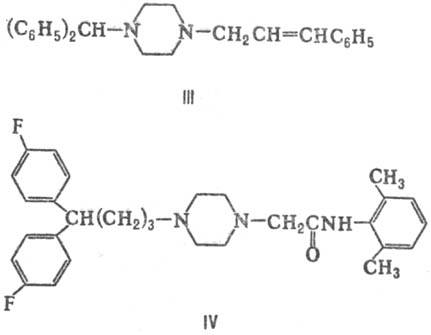
A number of myotropic antispasmodics has an elect. action on the tone of smooth muscles of certain organs or vascular areas. Among them, we distinguish w-va: coronary dilating (antianginal w-va, coronary lytics), improving cerebral and peripheral. (peripheral vasodilators) blood circulation, bronchodilators (bronchodilators, bronchodilators), lowering the tone of the uterus (to-colytic agents), etc. Coronary dilating antispasmodics are org. and inorg. and -nitroglycerin, C 4 , (V), (CH 3) 2 CHCH 2 CH 2 ONO, NaNO 2, etc. Most of the drugs in this group are used in the form of the so-called. prolonged lek. forms, to-rye gradually isolated in the active in-in. Spasms of the brain reduce, in particular, derivatives of vincamine to-you - natural (devincan; VI) and synthetic (; VII). Peripheral vasodilators include the phthalazine derivative ( , or hydralazine; VIII) and Na 2 .
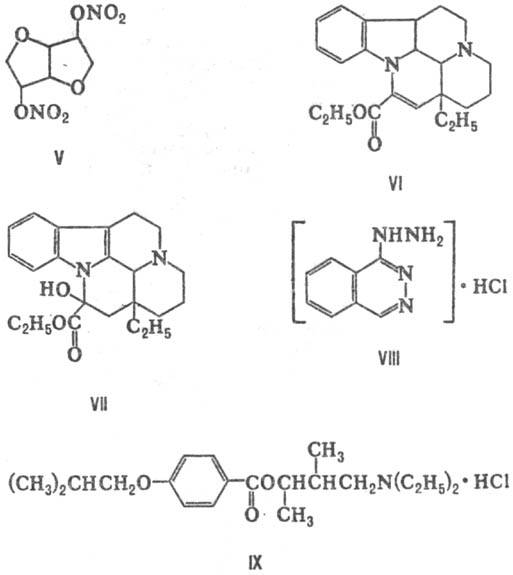
Non-selective myotropic antispasmodics include, for example, carboxylic to-t [ (C 6 H 5) 2 CHC (O) S (CH 2) 2 N (C 2 H 5) 2, (C 6 H 5) 2 CHC (O)S(CH 2) 2 N(C 3 H 7) 2 , (IX)], derivatives ( , ; X), (